Showing love and compassion for your eating disorder means you can actually change your relationship with it. In this episode of The Aleo Podcast, eating disorder clinicians Lee and Raquel challenge traditional perceptions of eating disorders being an evil adversary to overcome in battle and instead offer reframing eating disorders as painful parts of us with good intentions.
Lee’s perspective is informed by their work in IFS (Internal Family Systems therapy).
What is structured eating? And how do I know if it’s right for me and my recovery from disordered eating?
Join eating disorder clinicians Courtenay and Lee for a conversation exploring structured eating where they will help answer some of these common questions: What does structured eating even look like? And, how do I know I’m ready to move beyond structure?
Whether it’s aging, medical events, disability, or menstruation, our bodies are constantly changing throughout our lifespan. And yet, we get suckered into believing that abnormal or not okay. What’s that about?
In this pilot episode of The Aleo Podcast, eating disorder clinicians Raquel and Courtenay discuss the need to normalize the reality that bodies change. Raquel shares some of her personal story of navigating body image concerns following giving birth and provides insight on improving your relationship with your body through the lens of ACT (Acceptance and Commitment Therapy).
As originally seen here, September 2025, in: Connection Magazine, a publication by the Nova Scotia College of Social Workers
Conversations about food, weight, and bodies show up more often in practice than we might expect. As a Registered Dietitian who works closely with individuals in eating disorder recovery, I know firsthand how much a provider’s language and cues can shape a client’s sense of safety. Before we can support clients struggling with food and body concerns, we need to reflect on our own beliefs.
Now of course, I’m writing this as a dietitian who inherently will be talking about food much more directly than most social workers. And it’s important for my social worker colleagues to recognize that even when there’s an RD on the team, the way you talk about (or avoid talking about) food and body still matters — your words can either reinforce shame or open the door to healing. In this article, I’ll share more about how to examine our own biases around food and body, what that means for our clients (with and without eating disorders), and how to move forward while upholding dignity and safe practice.
Self-reflection
Let’s take a moment to do your own self-reflection about food and body. You might want to pull out a pad of paper for these questions. Before we get started, it’s important to know that how you approach clients (with or without eating disorders) can be influenced by your own relationship with food, body image, and assumptions about health. Now, take a moment to reflect on these key questions:
How has your relationship with food and your body influenced how you view and work with clients as a social worker?
Have you ever made assumptions about a person’s health or behaviours based on their weight? How could this affect your care?
How do you interact with people in larger bodies? Do you notice any differences in how you approach folks in smaller bodies vs larger bodies?
Why does self-reflection about food and body matter?
As all good social workers already know, self-reflection is the practice of examining your own assumptions, biases, and lived experiences, and considering how they influence your work. When it comes to food and bodies, this becomes especially important. We all live in a society obsessed with diet culture, where we are saturated with messages about dieting, “healthy” eating, and weight loss. Unfortunately, these messages disproportionately harm folks in larger bodies and can spur and perpetuate disordered eating, sometimes leading to a diagnosable eating disorder. These beliefs can shape the way we, as clinicians, view and respond to our clients.
For example, I’ve had clients who were told to “just lose weight” when they expressed feeling unhappy about their body size. Perhaps this clinician has engaged in dieting themselves, and they believe it’s something that “works” for everyone. This advice may have been well-intentioned, based on the belief that weight loss can resolve poor body image. In reality, research shows that 95-98% of weight loss attempts through dieting are not sustainable. And importantly, weight loss does not resolve body image distress in the long term. In my experience, clients who are told to lose weight have usually already tried this — often dozens of times. They’ve tried fad diets, “watching what I eat,” calorie counting, exercise. None of this is new to them. Telling someone to lose weight, especially without understanding their relationship with food, access to food, and beliefs about body size and health, can quickly become the catalyst for an unhealthy relationship with food, or even the onset of an eating disorder.
Research shows that weight stigma in healthcare, like in the example above, is linked to poorer health outcomes, increased shame, and barriers to seeking support. Given that eating disorders affect nearly 2 million Canadians (and disordered eating is even more widespread), every interaction matters.
For anyone wanting to dig deeper into understanding their own attitudes and beliefs about weight, I highly recommend taking the Weight Implicit Association Test (IAT). By examining your own biases, you are taking an important step forward to reducing the negative effects of diet culture, weight stigma, or shame in your work. You also create a safer environment for clients to share their experiences openly. This is particularly vital for clients living in larger bodies, for those with eating disorders, and for anyone navigating body image distress.
What this looks like for you and your clients
When I reflect on my own journey as a clinician (specifically as a Registered Dietitian who now works in the eating disorder field), I see how my personal relationship with food and my body influenced the way I showed up for clients early on. It’s uncomfortable work, and being willing to learn and unlearn these biases has helped me offer care that is both more compassionate and more effective.
For social workers, this self-awareness strengthens your therapeutic presence. It helps you recognize when a reaction may be about your own internalized beliefs, rather than your client’s needs. It also creates more room for curiosity — try asking yourself, “how is food showing up in this person’s life?” instead of making assumptions.
Imagine the incredible shift that can take place in your client interactions when you start asking questions like:
“What was food like for you growing up?” – This can be a powerful question to explore.
“What does ‘healthy eating’ mean to you and your family?” – There is no one specific way to define ‘healthy eating’, meaning it will look different from one person to the next.
“What kind of resources do you have to access food?” – This may reveal food insecurity, transportation limitations to acquire food, and barriers to cooking.
You might not have all the answers or know exactly what to do next, but holding space for a nonjudgmental conversation about food can go a long way and be an incredible foundation of rapport.
Actionable steps for clinicians
Working with eating disorder clients doesn’t mean you have to know everything, but there are clear steps you can take to provide meaningful support:
Learn as much as you can about eating disorders, disordered eating, and diet culture. Expand your knowledge by reading books like Sick Enough by Dr. Jennifer Gaudiani, Life Without Ed by Jenni Schaefer, and The Body Is Not an Apology by Sonya Renee Taylor. Food Psych by Christy Harrison is a wonderful podcast to learn more from. A great Canadian website about eating disorders that we often recommend is the National Eating Disorders Information Centre (NEDIC).
Self-reflect. Ask yourself hard questions. How do my own food and body experiences shape the way I see my clients? What words am I using to describe food? Do I describe foods as “healthy” or “junk”? Do I comment on body size, even casually? Remember, the way you talk about your own body and food habits can influence others.
Practice active listening, especially when exploring someone’s relationship with food and body. Validating a client’s feelings and experience can be incredibly powerful.
Collaborate with a team. You don’t have to know everything; the best care for eating disorders and disordered eating is often multidisciplinary. Work with dietitians, therapists, and medical professionals to ensure comprehensive care. If a client doesn’t have a team, help build a team or consult with other eating disorder professionals.
Refer when necessary. Know the options for higher levels of care and how to connect clients. If waitlists are long, continue supporting your client with compassion and harm-reduction strategies.
Advocate for your clients. Advocacy can make a huge difference, whether it’s within the healthcare system, with family members, or through education about eating disorders in your community.
The words we use, and how we talk about food and body, matter; they can either reinforce shame and stigma or open a space for curiosity, understanding, and healing. By bringing awareness to your own beliefs about food and bodies, you can reduce harm and create space for your clients with eating challenges to feel seen and supported.
Note: This blog post contains descriptions of disordered eating behaviours. A content warning is listed prior to that section.
When it comes to eating disorders, there is no shortage of fighting imagery. Beat it, conquer it, destroy it, defeat it. And before you read another word here, I first want to say: if those approaches work for you, or your loved one, or your client? Then keep doing them. I’m not trying to take this from you.
But for a lot of people, this approach isn’t working.
We know that many people never get treatment. And for those who do, they often don’t complete treatment. And even for those who do, there is a high rate of “relapse.” There’s no universally agreed-upon definition of recovery or relapse, so articles vary wildly in the numbers they quote, but everyone seems to agree that eating disorders are often a long-term struggle.
So, clearly, something isn’t working here. But why?
Maybe it’s because the eating disorder isn’t actually evil.
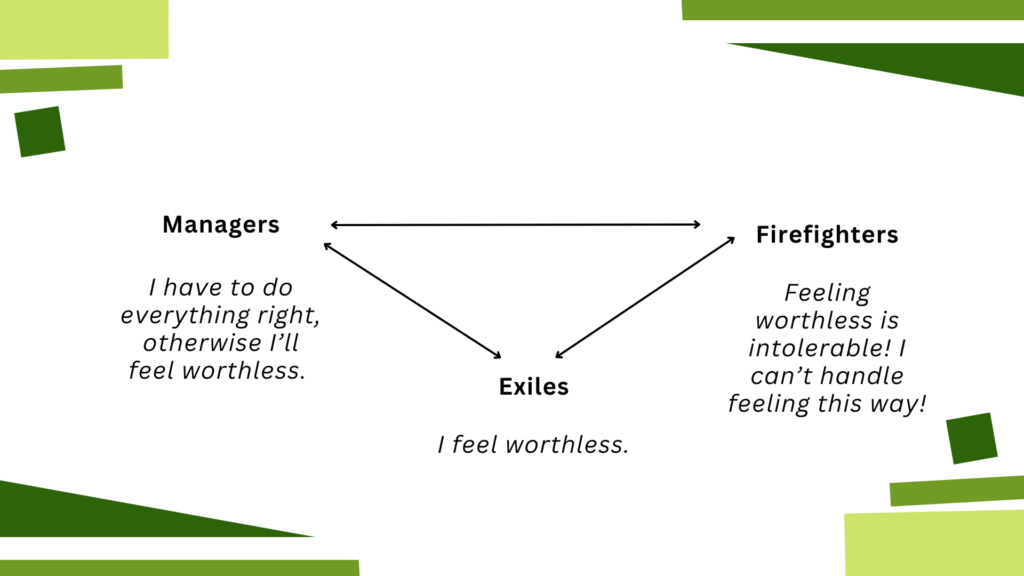
Enter IFS, stage left. Internal Family Systems therapy, or IFS, is based on the concept of multiplicity — that your mind isn’t all one thing, even though that’s what you’ve probably been taught most of your life. Instead, your mind is made up of a bunch of different subpersonalities, or “parts.” Sort of like the movie Inside Out, but for real. In IFS we divide these parts into 3 categories:
Exiles are generally young parts of us that hold a lot of big emotions, especially pain. This might be the part of us that says “I feel worthless”.
Managers are the proactive parts of us that try to prevent this exiled pain from overwhelming us. This might be the part of us that says “I have to do everything perfectly, otherwise I’ll feel worthless.”
Firefighters are the reactive parts of us that leap into action when the exiled pain is overwhelming us. This might be the part of us that says “I can’t handle feeling this way! I have to make it stop!” And will do whatever it takes to rescue us in that moment.
[Content warning: disordered behaviours. Skip this italicized section if you’d like to avoid]
In real life, this might look something like this: I might have an exile that believes that my body is bad and wrong, and feels a ton of shame whenever anything body-related comes up. In order to prevent this shame from flooding me, I might have a manager that says “if you just lose weight, then you won’t need to feel that shame.” And maybe it works, for a moment…
…But then, maybe I am rejected by a potential romantic partner, and I assume (rightly or wrongly) that it’s because of my body. The exile comes screaming out and starts to flood me with feelings of shame. It’s like an emotional fire that’s burning me up inside. It feels intolerable. So then a firefighter comes in to rescue me from this fire, and I scramble to the cupboard to eat anything I can get my hands on, whatever it takes to numb this horrible feeling.And maybe it works, for a moment…
…But then the manager voice comes back online and is horrified and critical: “I can’t believe you ate all of that! You’re disgusting! You’re a failure! No wonder nobody likes you!” This makes my exile start to feel shame again, and a firefighter comes back in to put out this new fire: get rid of the food. And maybe it works, for a moment…
…But then the manager criticizes me for throwing up and pledges that tomorrow we won’t let ourselves eat so much, because that’ll make up for today being such a disaster. And on, and on, and on.
So as you can see, the parts are trying desperately to help keep things stable in their own way — even though the ways in which they’re trying to help aren’t, in fact, helpful. Like many elements of disordered eating, it’s like being stranded in the middle of the ocean on a raft and drinking salt water to try to quench your thirst, even though it ultimately makes you more dehydrated. It’s an act of desperation that, despite being unhelpful in the long term, is entirely understandable given the circumstances. And, despite being entirely understandable given the circumstances, is also not helpful long term. Just because it hurts doesn’t mean it’s malicious, and just because it’s not malicious doesn’t mean it doesn’t hurt.
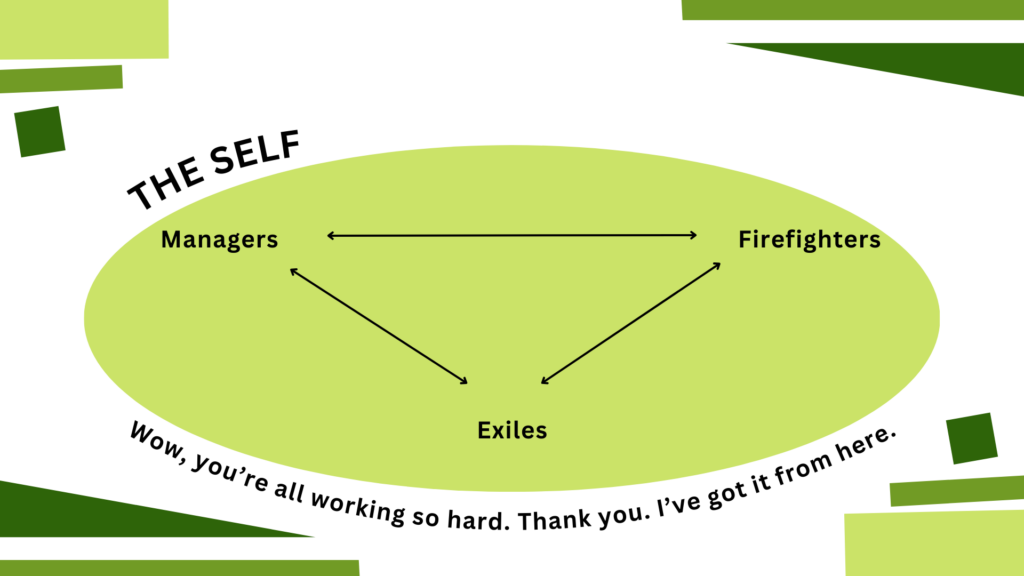
There’s another element at play as well, something that’s not exactly a part — your Self. One of the things that I like about IFS is also one of the things that I have struggled with the most about it, which is that it is unabashedly spiritual. IFS believes that everyone has a Self, which is sort of like a soul, or a core You.
This Self is like a compassionate, curious, loving parent figure. It knows that your parts are trying so hard to help you, that they actually kind of hate the job that they’re doing right now, and that they’re only doing it because they feel like they have to. We say there are No Bad Parts because the parts aren’t evil or malicious. They’re just extremely misguided. They are so good in their hearts, they are trying so hard to help, but they have very hard, and sometimes very harmful, jobs.
In our italicized example above, the exile part is holding onto so much pain related to shaming experiences around my body. The manager part wants to help prevent this pain, so they criticize me harshly before anyone else gets a chance to, even though they know it’s hurtful. The firefighter part doesn’t want to see me incapacitated by pain, so they try to help using the only tools available to them, even though this job earns them nothing but criticism from all the other parts (not to mention everyone else in my life). These parts are so profoundly dedicated to helping me, even at the expense of their own wellbeing. So then when outsiders like therapists and family members label these parts as “monsters” and “enemies,” no wonder they push back.
So if we’re not fighting them, what do we do instead?
It’s not easy, but it is simple. We love them.
If you rolled your eyes here, I feel you. There’s a part of me that genuinely can’t believe the type of therapist I am now. I can hear my younger self saying incredulously, “A key component to healing from an eating disorder is love? Grow up.” But unfortunately, it is true. I sometimes joke that I became an IFS therapist because at my heart I’m actually an ACT therapist — it’s all about workability for me, and this loving approach works.**
At its heart, IFS is about building community. Imagine if you felt like you belonged, and were safe, and unconditionally cared for. Imagine the sort of healing you could do if you felt like you were deeply loved no matter what. Imagine if someone saw the good in you even when you yourself can’t see it. That’s the power of community. IFS helps you to create that world internally, which can help you create it externally, too.
So what does that look like in real life?***
I might have an exile that feels a huge amount of shame about my body. I might work with this exile in therapy to help it to release the beliefs that burden it. I might help it get un-stuck from the past. I might let this exile know that I’m delighted by it, and that not only am I able to take care of them, but in fact I would be thrilled to take care of them.
I might have a manager that says “if you just lose weight, then you won’t need to feel that shame.” And I might sit with that manager and say “It makes so much sense to me that you feel that way. Thank you so much for trying to protect me.” I might help that manager to understand that I’m not a little kid any more, that they don’t need to take care of me. I might let this manager see that I care about my future and that they don’t need to be harsh in order for us all to be safe.
If my exile gets triggered and my firefighter comes in to rescue me, I might say “Wow. You are working so hard. Thank you so much. I’ve got it from here. I love that exile part, and its distress isn’t too much for me to handle.” I might let the firefighter see that I’m still engaging in pleasurable activities even when things aren’t on fire. I might tell them how much I appreciate all the things they’ve done to try to protect me over the years.
I do want to reiterate that being compassionate doesn’t mean that we’re enabling these parts. Loving a child doesn’t mean that we let them drive the car. But it does mean that we respond to them with compassion and kindness rather than with cruelty and punishment. We’re not fighting them because they’re not our enemy. We appreciate how hard they’re trying to help, and we recognize that they’ve been trying to help us for a long, long time. As Sam Dylan Finch wrote in this excellent blog post, “To relate to my ED as something I have to ‘fight’ or ‘beat’ is a betrayal of all the younger versions of me that conspired to protect my life and my future. I wouldn’t be here without them.”
Our parts love us deeply, and it’s about time we love them back.
If you’re interested in working with an IFS therapist, I recommend using the IFS directory or searching out someone who has received a minimum of Level 1 training from the IFS Institute. As of the time of writing this article I am not currently accepting new clients for individual therapy, but you’re always welcome to check my availability here to see if that’s changed. I do have spots available for clinical consultation.
* For the record, I think that the blog post on externalization that I pulled this quote from was very thoughtful and well-done, so I don’t mean for this to be perceived as a criticism of the blog post itself
** IFS is not a new therapy, but it is having a very hot moment right now, so lots of people are hearing about it. In some ways, I love this — I think IFS is great, and I have personally and professionally experienced how powerful it can be. But I feel like it’d be remiss not to note that so many therapies have had this same arc. Therapeutic modalities can be trendy just like anything else. So do I think IFS is amazing and a therapeutic modality well worth considering? 100%. But do I think it’s a perfect panacea and the only possible route to healing? Absolutely not.
*** If these examples sound trite or corny, I get that. Taking this stuff out of the individual therapeutic context has that effect, but I felt like I should include some examples anyway. Please trust me when I say that if you do this work with your own parts, the compassionate statements you come up with will not feel corny at all.
Last year, Raquel and Lee contributed to the “Queerly” project in collaboration with TransCare+. We wanted to share this very cool resource with you and summarize our specific contributions:
Queerly Volume 1 is an anthology exploring the intersections of queer identity, community, and ecology through the themes of “Grow,” “Eat,” and “Live.” Developed by queer and gender-diverse voices across Canada, the book combines storytelling, art, activities, and poetry to celebrate the resilience and creativity of 2SLGBTQIA+ communities. With contributions ranging from tattoo art and gardening guides to reflections on communal care and food as resistance, the collection fosters a sense of belonging and encourages readers to engage with nature and their surroundings in radical, affirming ways.
Queerly Volume 1 is an anthology exploring the intersections of queer identity, community, and ecology through the themes of “Grow,” “Eat,” and “Live.”
(if you’re having difficulty accessing the resource, email us thealeocollective@gmail.com and we’ll email you a PDF version!)
“Eat”, the section that begins on page 55, is the section Raquel and Lee contributed to:
Page 60: “Queering food and eating” audio recorded conversation This conversation between Lee Thomas and Raquel Griffin explores the intersections of queerness, food, and eating practices, focusing on how queering food systems can foster inclusivity, and challenge societal norms. The dialogue emphasizes the cultural, political, and personal dimensions of food as a site of resistance and identity.
Page 61: Visual ecosystem map (by Lee Thomas) Walks you through creating your own visual ecosystem map of your relationship with food/eating
Page 64: What do you really want to eat? (By Raquel) Using Intuitive Eating principles, Raquel walks you through a mindful eating experience, exploring the sensory aspects of food to assist you in exploring the question “What do you really want to eat”? Available through multiple mediums: a guided audio practice, transcript from the audio practice, or through provided journal prompts.
As a dietitian focusing on eating disorder care, I’ve worked with individuals with many different challenges with food. And a common theme we focus on, especially early on in our nutrition counselling together, is this idea of structured eating.
If you’ve ever struggled with disordered eating, an eating disorder, or years of dieting, you know that hunger and fullness cues can become unreliable. Maybe you’re not sure when you’re hungry, or you wait until you’re starving, which can sometimes lead to overeating or binge eating. Sometimes those cues are absent completely, making it difficult to eat anything. Other factors like gastrointestinal issues, medications, low mood, and more can greatly impact our ability to tune into our body and know how to feed it. This is where structured eating comes in.
Also known as scheduled eating, mechanical eating, or nutrition rehabilitation, structured eating helps to support regular eating patterns to meet your body’s nutritional needs (even when you’re unsure of your hunger and fullness signals).
Why Structured Eating?
This is my favourite analogy: think of structured eating like a cast on a broken arm. When your body is healing, you need extra support to keep everything in place. Over time, the cast comes off, and in time, you may start to use your arm more intuitively again. The same is true for your eating habits. When you’ve been struggling with an eating disorder of any kind or even chronic dieting, we’re probably going to need some sort of structure to support you nutritionally while you are working on healing your relationship with food and body. Structured eating provides the foundation you need while you heal, helping you establish a rhythm of consistent meals and snacks so that eventually, you can tune back into your body’s natural hunger and fullness cues.
The Basics of Structured Eating
Structured eating doesn’t mean following rigid rules or feeling restricted. Instead, it’s about creating a pattern of eating that allows your body to trust that it will be fed regularly and adequately. Think of structured eating like a blueprint, or rough guideline to support regular eating for recovery. Some people may require more details with their structured eating plan, and for others, it will be more flexible. Here are the key elements I like to focus on with my clients:
3 meals a day Aim for three meals, or “eating moments”, every day. For some, this might look like breakfast, lunch, and dinner. Focusing on getting at least 3 eating moments can help anchor your day and give your body regular fuel.
2 – 3 snacks a day Include smaller eating moments between your main meals. These snacks help keep your energy stable and prevent feeling overly hungry by mealtime. Snacks can help sustain you and keep blood sugar levels more stable between meals.
Include 3 or more food groups at meals Generally, a meal should have representation from several different food groups in order to provide us with a combination of carbohydrates, protein and fat (our three macronutrients). Try to include at least three different food groups at each meal (or larger eating moment).
Aim to eat roughly every 3 hours All human bodies will do best when fed regularly and adequately. Consider the timing of when you eat, aiming not to go beyond 3 hours between eating moments. It is absolutely okay to eat more often than this if that’s what you body needs and wants. Going many hours between eating can be harder physically on the body, and can negatively impact things like mood, blood sugar levels, energy, and sometimes perpetuate disordered eating behaviours.
Getting Started with Structured Eating
Starting structured eating can feel like a big change, especially if you’ve been stuck in a cycle of restriction or binge eating. Here are a few gentle tips to ease into it:
Start small You don’t have to change everything at once. Pick one aspect to focus on at a time, such as aiming to eat 3 times/day. Once that feels comfortable, add in snacks and consider the timing.
Set reminders It’s easy to forget to eat, especially if you’re used to skipping meals. Set alarms or reminders on your phone to help keep you on track with regular eating times.
Plan ahead You don’t need an elaborate meal plan, but having a list of go-to meals and snacks can make eating regularly much easier. Keep it simple and focus on what feels doable for you.
Track your progress Notice how you feel as you start to establish these regular eating habits. Are you more energized? Less likely to binge? If you miss a meal or snack, or have a binge, this doesn’t take away the fact that you are taking steps forward with your recovery. Healing is a process (and not a linear one at that). It’s often about baby steps!
Be kind to yourself If things don’t go perfectly, that’s okay! Self-compassion is HUGE when working on your nutrition for recovery.
Get support Structured eating is a powerful tool, but sometimes having guidance from a trusted support can be help. Working with a dietitian or healthcare provider can make the process easier and give you the support you need.
Remember: Food Has No Morality
One of the most important things to understand is that food has no moral value. There are no “good” or “bad” foods. Whether it’s kale or a cupcake, there is nutrition to be had and it doesn’t define your worth. Every food has its place, and structured eating helps you embrace a diverse range of foods with less guilt and more confidence that you are giving your body what it needs.
What would it be like to start working on implementing structured eating today?
Note: Many Aleo blog posts are meant to be read by clients who are struggling with disordered eating or body image concerns. This one, though, is specifically for clinicians. (But of course anyone is welcome to read it!)
In my therapy practice, many people I work with have sought me out specifically because of my eating disorder specialization, which is probably not super surprising. Want therapy for an eating disorder, see an eating disorder therapist.
But a lot of clients I’ve worked with over the years didn’t come in initially for eating disorder therapy. They came in for other concerns — alcohol use, relationship problems, childhood trauma, work stress, ADHD management, you name it — and then in our work together we discovered that they have a disordered relationship with food. My secret strategy for uncovering this? I ask.
“What is your relationship with food?” is a pretty standard question for me to ask within the first session or two. If the client answers in a way that suggests a disordered relationship with food, usually my followup question is “have you ever talked about this with a therapist before?” What I’ve found surprising is that the answer is almost always no… even when it’s a client who had already been in therapy for many years.
Now, to be clear, this isn’t meant to be a shaming “gotcha!” to you or any other clinician. Clinicians are fallible, myself included. We all bring our own lenses into this work — and we don’t tend to find what we’re not looking for.
“I don’t work with eating disorders” is a common thing for me to hear therapists say. But this creates a vicious cycle where clinicians believe they don’t work with clients with eating disorders, and so don’t ask their clients questions about eating disorders, and so they don’t hear about their clients’ eating disorders, and so they continue to believe that they don’t work with clients with eating disorders.
And obviously nobody is required to change their practice in any way just because I wrote a blog post. But what I’m hoping to do here is to help clinicians recognize that 1) yes, you can work with clients with eating disorders, and 2) you don’t have to do it alone.
To start with, let’s name some concerns that you, as a clinician, might have about working with clients with eating disorders.
“I need to work through my own food stuff first!”
You might have your own disordered relationship with eating and not feel like you’re in a place where they can effectively work with others around this topic. Even though you’re a clinician, you are a person first, and it’s absolutely okay to be selective about your work in order to keep yourself well. That being said, I don’t think your own disordered relationship with food inherently precludes you from being a good therapist to others. My own early work in the mental health field was as a “person with lived experience” (as we called it back then), and there’s lots of good work by Dr. Jennie Wang-Hall on this topic as well. Having support through something like a clinical consultation group can help you to explore things like countertransference to help ensure you’re taking care of both yourself and your clients.
“Clients with eating disorders don’t want to change.”
There’s still, unfortunately, a lot of stigma around people with eating disorders. Clients with eating disorders are still sometimes portrayed as manipulative, untrustworthy, unmotivated, and resistant. Can they be those things? Sure. They are human beings. We are all capable of being those things, sometimes. But a lot of this stigma is based on carceral beliefs about mental health care provision, and it’s not true.
In defence of most clinicians, in my experience the percentage of clinicians who don’t work with clients with eating disorders because of overt stigma is actually pretty low. (Or maybe that’s the circles I run in, because the researchdefinitelyreflects that stigma is still very much present.) But none of us are infallible, and it can be easy to slip into stigmatizing beliefs if you’re not surrounded by a community of clinicians who can support you when you’re feeling discouraged, and lovingly hold you accountable when you start to veer off course.
“There’s too many liability concerns.”
I’ve been in a lot of clinician consultation groups, and a common thread that I hear is that we as clinicians are terrified of getting in trouble, whether that’s with our college or with the legal system. In a lot of ways this can be a good thing — we have a lot of power in the therapeutic relationship, and having the college as an institution to protect the public helps to ensure that health care professionals are behaving ethically. However, I do think that sometimes the fear of getting in trouble becomes a sort of boogeyman that causes clinicians to be more risk averse than is necessary, even when it’s to the client’s detriment. We’re so afraid of doing the wrong thing so we end up doing nothing! And eating disorders can exacerbate this risk aversion because of the physical health concerns involved. Part of the benefit of a consultation group is that you can explore your concerns with other professionals, who can help you to figure out which risks feel worthwhile.
“It’s outside of my scope.”
I think there’s a both/and to be had here. On the one hand, it’s really important to practice within our scope and training. Like, I don’t have any EMDR training, so it would be wildly unethical if I were to just start doing EMDR (especially if my only motivation was that some random person wrote a blog post telling me that I should). But on the other hand, I think it’s also important to acknowledge that part of how we expand our scope is by pushing into new areas where we are not yet an expert.
I think this is especially true for clients where you already have an established relationship. Researchconsistentlyshows that the biggest predictor of positive therapeutic outcomes is the relationship between the client and the clinician. You might not be an eating disorder expert, but you might be a Therapeutic Alliance With This Specific Client expert, and that’s a really, really important element to consider. If you’re considering expanding your scope in order to support an existing client, consultation (whether individual or group) is definitely something you’ll want to pursue to help you increase your clinical skills and steer clear of potential pitfalls.
“I only work with trauma (or anxiety, or substance use, or…)”
This is a variation of the “scope” concern, I think. And, again, if you really want to stay in your specific wheelhouse, nobody is stopping you. But there’s a ton of comorbidity with eating disorders and other conditions. If you’re working with trauma, or anxiety, or substance use, or almost any other area, you are almost certainly also working with clients with eating disorders. And that’s even before we consider the subthreshold eating disorders, aka disordered eating. Food is one of the basic building blocks of the human experience — it’s going to influence, and be influenced by, other conditions in a client’s life. If someone has experienced trauma we aren’t shocked when it impacts their relationship with romantic partners, friends, work, or many other elements of their life. We should expect that it would impact their relationship with food, too.
So all of this to say: the reality is that you’re already working with clients with eating disorders. The choice you have now is what you want to do with this information.
As a clinician in a private practice, I’ve made a point of investing in consultation throughout my career, and I truly can’t overstate the impact that it’s had on my practice. A consultation group is a soft place to land when you’re feeling discouraged, and it’s a reality check when you’re way off track. It’s a place to learn strategies and phrases that your colleagues find helpful with their clients. It’s a source of reassurance and guidance. And, as a bonus, it’s often counted as continuing education credits.
Courtenay Vickers is a registered dietitian and member of the Aleo Collective. She and I decided to start this group because we’ve both found consultation to be unbelievably valuable to ourselves, our practices, and our clients — and we want to share it with you!
Registration for our group closes January 31, 2025. We would love for you to join us!
Written by: Raquel Griffin MSW RSW Time to read: 5 minutes
Sinful snacks, cheat days, and junk food— oh my!! These phrases probably sound pretty familiar; they demonstrate some of the ways in which diet culture’s flavours of puritanism, morality, and virtue are baked into our common discourses surrounding food and eating.
Historically, religion has long shaped the way we think about food and our bodies. Religions issued warnings about gluttony, engaging in fasting practices and avoidances of what could be seen as indulgent. These practices weren’t about weight loss for its own sake or the effects of eating on a person’s size, but about how bodily pleasure was thought to compromise the soul. It was penance: a way of making up for all the times you had screwed up that year, rather than a way of punishing your body for being too large.
Early Protestant Christianity associated bodily pleasure with moral weakness, emphasizing restraint and self-discipline as pathways to spiritual purity. Protestant Christian clergy and leaders like Sylvester Graham and John Harvey Kellogg were pioneers of so-called “healthy eating”, linking bland diets to moral and sexual chastity; this included their own inventions of the Graham Cracker and Cornflakes. Graham believed that all of America’s moral failings could be traced back to “unholy” ways of eating, which could be cured with a strict diet. Graham’s list of “excess” of sinful indulgences included: meat, spices, caffeine, alcohol, and warmed/heated food, to name a few. He even instructed his followers to abstain from dancing (“Footloose” style), to take cold baths, and sleep on hard beds. These practices weren’t merely about health—they were about control and conformity.
While some of these diets would be seen as overkill today, their legacy persists in modern diet culture’s manifestations, emphasizing individual responsibility which equates thinness with virtue and fatness as a moral failing. In practice, this looks like promoting restrictive eating as a marker of self-worth, abstaining or using “caution” with demonized foods, and pathologizing fatness as inherently diseased and wild. Diet culture’s obsession with categorizing foods as “good” or “bad” not only distorts our relationship with food but also fuels systemic oppression. It marginalizes those who don’t fit its narrow ideals, often targeting women and femmes, racialized folks, queer folks, disabled and those in larger or fat bodies. These standards are rooted not in health but in control—diet culture is a system of oppression, in all its facets.
Reclaiming Pleasure with Intuitive Eating Intuitive Eating principles offer a roadmap for this reclamation like rejecting the diet mentality, honouring hunger, making peace with food, and discovering the satisfaction factor.
Unconditional Permission to Eat Instead of viewing food as an enemy, allow yourself to enjoy it— label guilt as such when you notice it. You’ll notice that when you embrace variety and remove restrictions, food eventually loses its “forbidden fruit” allure.
Discover the Satisfaction Factor Tune into your senses: what flavours, textures, or aromas do you truly enjoy? Eating with intention—savouring each bite and minimizing distractions—can transform meals into moments of joy.
Create Joyful Food Memories Food doesn’t solely meet physical needs but also serves as a source of emotional and social connection. It brings people together, creates traditions, and tells stories. Recognizing these facets helps us see food as more than calories or nutrients—it’s a part of life’s richness. Make meaningful connections to memories involving food that were joyful. Who were you with? What made the experience special?
Reclaiming pleasure in food is an act of resistance against diet culture and the oppressive systems that sustain it. By rejecting rigidity, embracing flexibility, and reconnecting with ourselves, we can rediscover the joy and pleasure that eating was always meant to bring. A parting invitation: take that treasured creation of Sylvester’s Graham cracker and squish between two of them a warm, toasted marshmallow and melted chocolate square… Mmmm… what a delicious “Fuck you” to diet culture.
References:
Carlton, G. (2022, February 2). Meet sylvester graham, the religious health nut who thought white bread was evil. Retrieved from: https://allthatsinteresting.com/sylvester-graham
Look, M. (2024, February 12). Why was cereal invented? A brief history of corn flakes. Retrieved from: https://history.howstuffworks.com/american-history/why-was-cereal-invented.htm
Harrison, C. (2019). Anti-diet: Reclaim your time, money, well-being, and happiness through intuitive eating. Little Brown: UK.
Harrison, C. (2019, May 20). Episode#196: diet culture’s racist roots with Sabrina Strings. Food Psych. Retrieved from https://christyharrison.com/foodpsych/6/the-racist-roots-of-diet- culture-with-sabrina-strings-sociologist-and-author-of-fearing-the-black-body
Harrison, C. (2018, August 10). What is diet culture? Retrieved from: https://christyharrison.com/blog/what-is-diet-culture
Smith, A. F. (2009). Eating history: 30 turning points in the making of American cuisine. New York: Columbia University Press.
Strings, S. (2023, May 6). Fatphobia as misogynoir: gender, race & weight stigma. Body Talks Conference, Untrapped Academy.
Strings, S. (2019). Fearing the black body: the racial origins of fatphobia. New York University Press: New York.
Tribole, E., & Resch, E. (2020). Intuitive eating: A Revolutionary Anti-Diet Approach, 4th ed. St Martin’s Publishing Group: New York.
Tribole, E., & Resch, E. (2017). The intuitive eating workbook: ten principles for nourishing a healthy relationship with food. New Harbinger Publications: Oakland.
Written by: Courtenay Vickers RD Time to read: 6 minutes
For many healthcare providers, the thought of working with a client who has an eating disorder can be daunting. Questions like What if I say the wrong thing? or What if I make things worse? are common, and this uncertainty can make clinicians hesitate or feel stuck. With some practice and guidance, effective communication and building rapport can be life-changing for that client sitting across from you!
This blog post offers some helpful strategies for having compassionate conversations with eating disorder clients, integrating self-reflection, examples of what to say and what to avoid, and actionable steps for clinicians to build their confidence in this area.
Before we dig in, an invitation to remain curious rather than judgemental about your current/past self! Wherever you are at on your learning journey, that is ok. And I’m so glad you stumbled upon this post today.
First, what’s the difference between an eating disorder and disordered eating?
It’s important to recognize that there is a difference between an eating disorder and disordered eating when working with clients:
Eating Disorders are diagnosable mental health conditions outlined in the DSM, including:
Anorexia Nervosa (AN)
Bulimia Nervosa (BN)
Binge Eating Disorder (BED)
Avoidant/Restrictive Food Intake Disorder (ARFID)
Other Specified Feeding and Eating Disorders (OSFED)
Disordered Eating refers to a broader range of harmful eating patterns or behaviours that don’t meet diagnostic criteria but can still significantly affect physical and emotional health. Disordered eating can be a precursor to an eating disorder. Sometimes disordered eating looks like someone going on a diet, actively pursuing weight loss through dietary restriction, or even being “watchful” of what they eat. It’s not something to ever brush past.
With nearly 2 million Canadians affected by eating disorders—and the second-highest mortality rate among mental health conditions—it’s critical for clinicians to be prepared to address these complex issues with care and sensitivity.
Self-Reflection: Starting with Yourself
Let’s take a moment to do a little self-reflection. You might want to pull out a pad of paper for these questions. Before we get started, it’s important to know that how you approach eating disorder clients can be influenced by your own relationship with food, body image, and assumptions about health. Now, take a moment to reflect on these key questions:
How has your relationship with food and your body influenced how you view and work with clients as a healthcare provider?
Have you ever made assumptions about a person’s health or behaviours based on their weight? How could this affect your care?
How do you interact with patients in larger bodies? Do you notice any differences in how you approach patients in smaller or very thin bodies?
Self-awareness is vital. Recognizing and addressing personal biases is an important step toward creating an environment of trust and support for your clients.
Let’s explore some examples of what to say (and not to say)
Compassionate communication can make a significant difference in how clients feel about their care and recovery. Here are examples of what to avoid saying, along with alternatives that foster trust and understanding:
Instead of: “Just eat!”
Try: “It seems like eating is difficult for you. Tell me more about what challenges come up for you with eating.”
Instead of: “You don’t look like you have an eating disorder.”
Try: “Eating disorders can affect anyone, any age, any gender, any body size. Your experience is valid.”
Instead of: “You’re just going through a phase. Everyone feels insecure about their body sometimes.”
Try: “I imagine what you’re going through is incredibly difficult.”
Instead of: “Your vitals and blood work are fine; you don’t need to worry.”
Try: “Your body is working hard to keep things medically stable right now. I know other behaviours are going on, so let’s explore ways to better support you and reduce harm.”
Instead of: “I wish I had your self-control!”
Try: “The eating disorder is not your fault. It’s a complex brain-based illness, and you deserve to receive supportive care.”
Instead of: “You look healthy/better.”
Try: “How are you feeling about your recovery journey so far?”
Instead of: (silence)
Try: “I’m concerned about your eating. I’m wondering if we can explore your relationship with food a bit more together.”
Instead of: “Don’t worry, you’re not fat! You won’t get fat.”
Try: “I can imagine the idea of gaining weight feels scary for you. That makes sense, given how focused our society and healthcare system are on weight loss. Regardless of your body size, you are deserving and worthy of recovery.”
Instead of: “You have an eating disorder? Sorry, I can’t help you.”
Try: “It sounds like you’re having some real challenges with food and eating. You deserve proper care and support. Are you okay if we talk more about some options to help you?”
Actionable Steps for Clinicians
Working with eating disorder clients doesn’t mean you have to know everything, but there are clear steps you can take to provide meaningful support:
Practice Active Listening Listening without judgment or a need to immediately “fix” can be a powerful tool. Validating a client’s feelings and experience can make them feel seen and understood.
Collaborate with a Care Team Eating disorder treatment is often multidisciplinary. Work with dietitians, therapists, and medical professionals to ensure comprehensive care. If a client doesn’t have a team, help build a team or consult with other professionals on behalf of your client.
Refer When Necessary Know the options for higher levels of care and how to connect clients. If waitlists are long, continue supporting your client with compassion and harm-reduction strategies while they wait.
Advocate for your clients Advocacy can make a huge difference, whether it’s within the healthcare system, with family members, or through education about eating disorders in your community.
Building Confidence Through Practice
Feeling confident in conversations about eating disorders takes practice and support. If you want further guidance, consider joining Confident and Competent: Eating Disorder Clinician Consultation Group, starting in February 2025. This program offers group calls, practical skills, and a supportive community to deepen your expertise. Email us at thealeocollective@gmail.com to learn more and get on the waitlist.
Remember, you don’t have to be perfect or have all the answers to make a positive impact. By showing up with compassion, humility, and a willingness to learn, you can help clients feel supported and valued on their recovery journey.
Join our mailing list!
We promise to never spam you or sell your information. You can unsubscribe at any time.